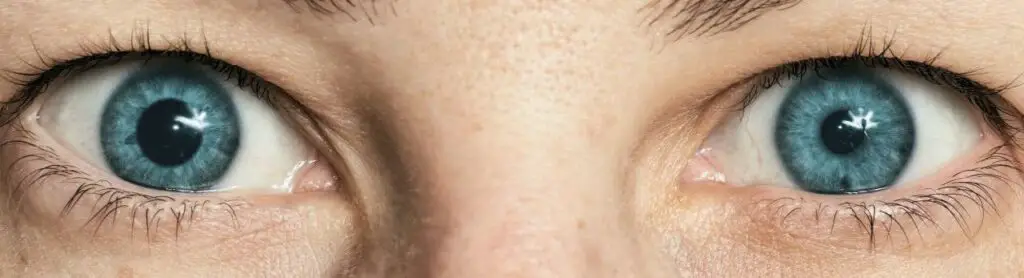
Look closely at your eyes in the mirror. Does one pupil appear noticeably bigger than other? If so, then you may have anisocoria.
Table of Contents
What is anisocoria(One pupil bigger than other)?

Simply put, anisocoria is when one pupil look bigger than other. One pupil may be larger than normal or smaller than normal. As a result, there are different sizes of pupils. As a rule, the reaction of two pupils to light may or may not be normal.
In most cases, anisocoria is a benign disease, so there is no cause for concern. However, if your pupils are suddenly unequal in size, it means that you have a rare form of anisocoria, which can be a symptom of a serious illness.
Types and causes of anisocoria (One pupil bigger than other)
There are four main types of anisocoria:
simple anisocoria.
pathological anisocoria.
mechanical anisocoria.
pharmacological anisocoria.
Simple anisocoria
Simple anisocoria, also called essential anisocoria or physiological anisocoria, is the most common type of anisocoria (One pupil bigger than other). It is a benign (harmless) eye condition that affects approximately 20% of the population.
In simple anisocoria, the difference in pupil diameter is usually 1 millimeter (mm) or less, and both pupils respond normally to light. It turns out that the presence of simple anisocoria does not depend on gender, age or eye color.
The exact cause of the development of simple anisocoria has not been established. It can be temporary or permanent, and sometimes goes away on its own.
Pathological anisocoria (One pupil bigger than other)
With pathological anisocoria, different pupil sizes (when one pupil bigger than other) are due to the presence of an underlying disease or a health disorder. as the following examples:
Irit
Iritis is a form of uveitis (an inflammatory eye disease). Acute iritis is characterized by redness and pain in the eyes, photophobia, inflammation in the anterior part of the eye, and constriction of the pupil of the affected eye (resulting in anisocoria).
There are many causes of iritis, including eye infections, underlying inflammatory conditions, and trauma. Your optometrist can treat the symptoms of iritis if the underlying cause is identified and controlled.
In some cases, anisocoria due to iritis may still persist, even with successfully treated iritis.
Horner’s syndrome
Although signs and symptoms may vary from person to person, most people with Horner’s syndrome have the following three signs:
ptosis (drooping eyelid);
miosis (narrowing of one pupil, in connection with which anisocoria occurs);
face aridity (loss of sweating around the affected eye).
Horner’s syndrome can also be distinguished from simple anisocoria by the rate of pupil dilation in dim light. Normal pupils (including normal pupils that vary slightly in size) dilate for five seconds after the light in the room is dimmed. A pupil affected by Horner’s syndrome usually takes 10 to 20 seconds to dilate in dim light or in a darkened room.
Horner’s syndrome usually occurs as a result of some pathology, such as a stroke, tumor, or injury to the spinal cord. However, there are certain instances where the cause is unknown.
Adie’s syndrome (tonic pupil)
Adie’s syndrome (tonic pupil) is a dilated pupil caused by damage to the nerve fibers that control the muscles in the eye that constrict the pupil. The affected pupil also reacts poorly to light. Adie’s syndrome (tonic pupil) occurs predominantly in women aged 20-40 years, and in 80% of cases only one eye is affected. In most cases, the cause of Adie’s syndrome (tonic pupil) is unknown.
Paralysis of the third pair of cranial nerves
The third (III) pair of cranial nerves (also known as the oculomotor nerve) controls several muscles responsible for eye and eyelid movement, and also influences the muscle that changes the size of the pupil. Paralysis of the oculomotor nerve causes the pupil of the affected eye to dilate, resulting in anisocoria.
Along with anisocoria, paralysis of the third pair of cranial nerves frequently results in ptosis (drooping of the eyelid), “down and out” displacement of the eyeball in the affected eye, and accommodation problems (the ability of the eye to focus on nearby objects)
Causes of third cranial nerve palsy include pressure on the optic nerve from an aneurysm, tumor, or intracerebral hemorrhage. The occurrence of oculomotor nerve palsy in children can be caused by migraines and severe infections such as meningitis.
Mechanical anisocoria
Mechanical anisocoria is a different size of the pupils as a result of damage to the iris or its supporting elements. The occurrence of this type of anisocoria is due to trauma to the eye, complications of eye surgery (including cataract surgery), angle-closure glaucoma, and inflammatory diseases such as iritis and uveitis.
Congenital anomalies in the structure of the iris can also be considered the cause of mechanical anisocoria.
As the following examples:
Aniridia (complete or partial absence of the iris of one eye).
Coloboma (splitting in the iris from birth, in which the pupil looks like a “drop” or “cat’s eye”).
Pupil ectopia (a congenital pathological condition that causes displacement of the pupil and dislocation of the lenses of the eyes).
Tumors inside the eye can also lead to the development of mechanical anisocoria.
Pharmacological anisocoria
This type of anisocoria (different pupil size) occurs as a side effect of medications.
Selective serotonin reuptake inhibitors (SSRIs) used to treat depression have been identified as a possible cause of pharmacological anisocoria .
It has been shown that scopolamine-based transdermal patches used to treat motion sickness and nausea after chemotherapy can also lead to the development of anisocoria.
Some eye drops used for glaucoma can also cause anisocoria, especially if they are used to treat glaucoma in only one eye. Among these drugs, the following have been established: pilocarpine can lead to a decrease in the pupil of the eye being treated, and brimonidine and apraclonidine can cause an increase in the pupil of the eye being treated.
What to do if you have anisocoria?
If you notice a different pupil size in yourself or someone you know or relatives, you should immediately contact an ophthalmologist, especially in the following cases:
Dropped eyelid (ptosis)
Double vision
vision loss
Headache or neck pain
Pain in the eye
Recent head or eye trauma
If the anisocoria is mild and your pupils respond normally during eye examinations, you may not need to worry. But to make sure you’re okay when your pupils are different sizes, you need to get tested.
If you have anisocoria and one pupil is larger than the other, ask your optometrist about photochromic lenses. These spectacle lenses will automatically darken when exposed to sunlight, thus reducing the sensitivity of your eyes to light (photophobia) that you may experience.
Photochromic lenses also protect your eyes from harmful UV rays and high-energy blue light, especially an eye with a dilated pupil that doesn’t respond normally to light.
You may are interesting in Sugar effect to the body | Very important




Thanks for sharing. I read many of your blog posts, cool, your blog is very good.
Your article helped me a lot, is there any more related content? Thanks!
Really enjoyed this!
Thanks for sharing. I read many of your blog posts, cool, your blog is very good.